Advances Across Ophthalmology: A Practical Guide to Geographic Atrophy, Ocular Surface Disease, Glaucoma, and Refractive IOL Surgery
Advances Across Ophthalmology
A Practical Guide to Geographic Atrophy, Ocular Surface Disease, Glaucoma, and Refractive IOL Surgery
The Clinical and Functional Burden of Geographic Atrophy
By Lejla Vajzovic, MD
Geographic atrophy (GA) is a major clinical challenge in retinal practice. As the advanced form of dry age-related macular degeneration (AMD), GA leads to irreversible and progressive loss of photoreceptors and retinal pigment epithelium (RPE), leading to functional vision loss that significantly impairs patient quality of life. For many, the disease threatens core aspects of independence. Patients experience broad functional impairment, including difficulty reading, reduced driving ability, challenges with daily activities, and reliance on visual aids.1
For many patients, the impact on driving is particularly significant. Among licensed drivers with GA, 50% and 88% reported lacking confidence driving during the day and at night, respectively. Most (82%) reported worsening vision over the past year compared with only 25% of controls (OR 13.55; P < .001).2 Loss of driving independence compounds isolation, limits access to appointments, and erodes the self-sufficiency that defines daily living for many older adults.
GA is also a heterogeneous disease. Progression rates vary substantially across patients, making it difficult to predict clinical course and determine the optimal timing of intervention. The variability highlights the need for consistent monitoring and systematic identification of patients at highest risk for rapid disease progression.
Several clinical parameters help guide risk stratification in practice. Lesion size at baseline is one of the most reliable predictors. Larger areas of GA at initial presentation correlate with accelerated future growth.3–5 Lesion pattern on fundus autofluorescence (FAF) is equally informative. High-risk FAF patterns, including banded and diffuse hyperautofluorescence at lesion borders, are associated with significantly faster growth rates (diffuse: 3.78 mm²/year; banded: 2.52 mm²/year) compared with focal or no hyperautofluorescence patterns (0.36 and 0.02 mm²/year, respectively).3,6
Multifocality is another key prognostic variable. Patients with multiple discrete GA lesions tend to progress more rapidly than those with unifocal disease.7 Extrafoveal and perifoveal lesion location, while often associated with preserved central acuity in the short term, carries its own prognostic concern because they typically expand faster than subfoveal disease, ultimately threatening the fovea.8 The status of the fellow eye also provides important context: When significant progression has occurred in a contralateral eye, symmetric behavior in a treated eye should be anticipated.4 Finally, tracking historical progression rates from prior imaging enables a more individualized forecast of where each patient falls on the progression continuum.5
On OCT, reticular pseudodrusen (RPD), characterized by irregularities above the RPE rather than the sub-RPE deposits seen with classic drusen, represent a high-risk biomarker for progression toward advanced disease.9,10 Their presence should prompt closer monitoring and consideration for earlier intervention.
CONCLUSION
Real-world integration of GA management requires both clinical acuity and honest acknowledgment of current barriers. Even with the recent expansion of approved therapies, early intervention remains underutilized. Therapy access and patient acceptance are among the most frequently cited barriers. These realities demand attention not only at the level of individual patient counseling, but in the broader systems and workflows that govern retinal care
Innovations in Earlier Detection
By Sophie J. Bakri, MD, MBA
The case for multimodal imaging in GA is straightforward. No single imaging modality provides a complete picture of disease status, progression risk, and treatment response. Each modality provides complementary information, enabling clinicians to move from descriptive assessment toward more predictive disease management.
FUNDAMENTALS FOR SUCCESS
Currently, OCT is the cornerstone of GA imaging and monitoring in most clinical settings. It enables direct visualization and quantification of structural changes central to GA pathophysiology, including drusen characterization, hyperreflective foci, ellipsoid zone (EZ) loss, and RPE atrophy (Figure 1).

Figure 1. OCT helps detect early structural changes associated with GA
OCT-derived quantitative metrics such as lesion size and the ratio of photoreceptor to RPE loss have emerged as important predictors of progression velocity and treatment response; a higher photoreceptor-to-RPE loss ratio is associated with greater responsiveness to complement inhibitor therapy.11
Incomplete outer retinal atrophy (iRORA) and complete outer retinal atrophy (cRORA) represent distinct structural stages on the OCT continuum whose differentiation carries both diagnostic and prognostic weight. Their classification should be based on careful structural assessment of retinal layers rather than transillumination profiles alone. Importantly, all major OCT platforms now include tools that allow clinicians to track lesion proximity to the fovea and monitor GA size serially. These images may be shown to patients to facilitate understanding of their disease trajectory.
Infrared imaging is a practical workhorse. Its ease of acquisition, compatibility with standard OCT platforms, and ability to clearly delineate GA lesion borders make it useful for serial monitoring and providing a retrospective window into disease history from archived imaging.
FAF adds critical information about lesion margin behavior (Figure 2). Hyperautofluorescence at the borders of a GA lesion signals metabolic stress in adjacent RPE cells and is associated with higher likelihood of near-term lesion expansion.3,6 FAF is particularly valuable in the context of multifocal disease, where it can help identify the full geographic distribution of atrophic areas. The stark hypoautofluorescence of atrophic zones also serves as a vivid and effective patient communication tool.
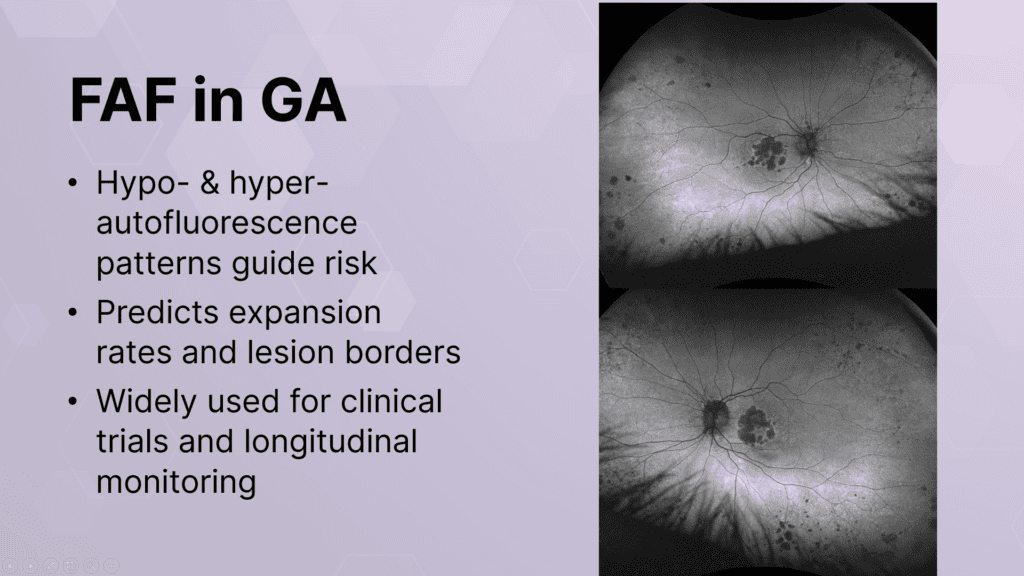
Figure 2. FAF helps predict lesion expansion rates and lesion borders.
Choriocapillaris flow deficits detectable on OCT angiography (OCT-A) represent an early biomarker for disease activity. The modality allows visualization of vascular alterations at the margins of GA lesions with predictive value for expansion rates.12 It can also serve as an efficient screening step to identify subclinical neovascularization before proceeding to fluorescein angiography (FA). This is an important consideration given that patients with GA face substantial risk of conversion to neovascular AMD.
Wide-field imaging complements macular-focused assessments. The imaging of peripheral GA lesions and subclinical changes outside the central field enable a more comprehensive survey of total retinal disease burden.
Emerging evidence suggests that GA may not be strictly a macular condition, and punched-out atrophic lesions can also appear in the retinal periphery, reflecting a broader pathophysiologic milieu that macular imaging alone may miss.13